Can Architecture Ever Save Us From Sickness?

A grid of empty white beds sits together in dark, cavernous spaces. Vast halls, centers, stadia, armories, and urban parks have been turned into field hospitals for thousands of the sick. These were the chilling scenes we saw all over the world during the early days of the COVID-19 crisis, from Belgrade to São Paulo and Mexico City to New York. And it was the same scenes we saw a century earlier, during a flu epidemic that, by some estimates, killed more people than the two world wars combined.

In health emergencies such as pandemics, we suddenly find that all buildings are medicalized: Large spaces become hospitals. Houses become quarantines. Every detail and use of every building is scrutinized in terms of sickness — and its prevention. Yet the needs of emergencies also eventually become inscribed into the everyday. Indeed, every architectural period has been shaped by a history of medical fears, misunderstandings, prejudices, inequities, and innovations.
It could even be argued that the beginning of architecture is the beginning of disease itself. As the physician Benjamin Ward Richardson put it when introducing “Our Homes and How to Make Them Healthy,” a compendium of texts by doctors and architects published for the 1884 International Health Exhibition in London: “Man, in constructing protection from exposure has constructed the conditions for disease.” In other words, all architecture is suspended between resisting and producing disease.
In ancient Rome, there was Vitruvius, who, in the first century BCE, established Western architectural theory by insisting that all architects study medicine: “Healthfulness being their chief object.” Indeed, a large part of his “Ten Books on Architecture” is devoted to the question of health. Vitruvius gives detailed instructions on how to determine the suitability of a proposed site for a city by returning to the ancient method of sacrificing a native animal and inspecting its liver to ensure it is “sound and firm.” Likewise, for the health of individual buildings, the text applies the theory of the four humors, the dominant medical paradigm of the time, to organize building orientation and ventilation. More striking, it argues that those who are deeply unwell, due to illnesses such as tuberculosis, can be cured through design.
This idea — that architecture can both prevent and cure disease — has persisted from the Late Middle Ages to the modern period, particularly in cities. In fact, urban environments represent an accumulation of theories of disease transmission and prevention. From new building types such as lazarettos in 15th-century Italy, designed to contain those infected or suspected of being infected with the plague, to the great infrastructure works of the 19th century — sewage systems, clean water, urban grids, and parks — cities have been completely reshaped in the name of health.
All architecture is suspended between resisting and producing disease.
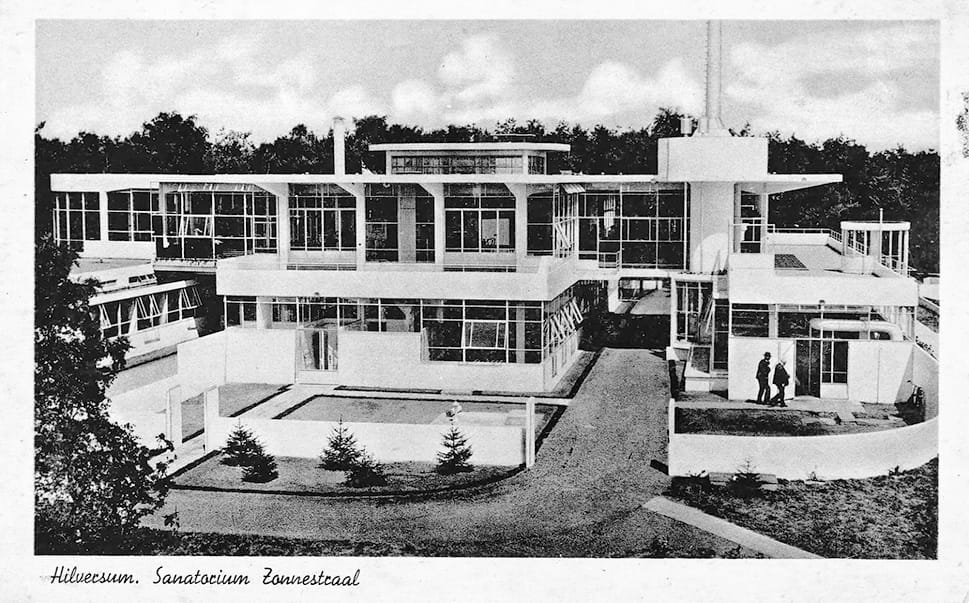
Throughout the late 19th and the first half of the 20th century, millions died of tuberculosis every year all over the world. Modern buildings offered a prophylactic defense against this invisible microorganism, the tuberculosis bacilli, which was only definitively identified in 1882. Features such as white walls, terraces, large windows, and detachment from the ground were presented as both prevention and cure. Yet the medicinal nature of modern architecture and the unimaginable horror it was responding to have been largely forgotten.
To convince the public that modern architecture was healthy, the decorative excess of 19th-century architecture was demonized as infectious and disease-ridden. Modern architecture was, on the other hand, a form of disinfection — a purification of buildings that would lead to an environment of light, air, cleanliness, and smooth white surfaces, without cracks or crevices where contagion might lurk. In periods when life expectancy was decades shorter, and most people died of bacterial diseases, modern architecture helped create a healthier environment. Yet like all antibiotics, it eventually created its own monsters.

Architecture produces sickness, most obviously sick building syndrome. For example, the air-conditioning systems that architects like Le Corbusier celebrated for isolating indoor air from contaminated outdoor air turned out to be reservoirs and vectors of disease. As in a science fiction horror film, the architecture that was supposed to inoculate its occupants against disease turned against them. Many of the diseases of our time, including obesity, diabetes, numerous cancers, autoimmune disorders, allergies, and possibly autism, are increasingly understood as the consequence of the diminishing diversity of bacteria.
Buildings have their own microbiomes, and the diversity of bacteria in buildings is just as important as the diversity of bacteria in bodies. But there is a crisis of diversity in this ecology. Just as modern architecture polemically reconfigured the 19th-century architectures that preceded it on health grounds, architecture today needs to be dramatically reconfigured in the name of newer health paradigms.
Ultimately, these reconfigurations are always political. They inevitably draw and maintain lines that privilege and shelter the privileged subject from threatening others. In reverse, to think in terms of sick architecture is to recognize that all borders, whether that of a room or a nation, are medical, particularly in instances of colonial power.
In the Belgian Congo, from 1908 to 1960, a 400-meter-wide band — the distance it was thought no mosquito could fly — separated the Indigenous city from the European city, supposedly to prevent yellow fever. The medical border acted as a mechanism of racialization, with mosquitoes dimensioning the city. The construction of the Panama Canal, too, was predicated on the conquest of the mosquito. It involved both large- and small-scale interventions, from the clearing of forests and draining of swamps to the installation of screened verandas and other architectural devices deployed along, and reinforcing, racialized lines.
Another wrinkle is that health has never just been physical. As early as ancient Greece, a variety of mental illnesses were identified and spatialized inasmuch as sufferers were forced to remain indoors or roam the outdoors without an address. Eventually, specialized buildings offered both isolation and care.
The diversity of bacteria in buildings is just as important as the diversity of bacteria in bodies.
The Muslim philosopher and physician Ibn Sina, who lived in the late 10th and 11th centuries, wrote about treating the “head sick” with calming gardens and fountains, drawing on a tradition of bimaristans — Islamic hospitals with dedicated wards for the mentally ill — that had emerged in Baghdad as early as the 8th century. The Hospital of the Innocents, considered the first psychiatric hospital in the Western world and a model throughout Europe and the Americas, was founded in Valencia in 1409, following observation of Islamic institutions in Ibn Sina’s mold. Eventually, much of the architectural effort to treat mental illness was undone by the anti-psychiatric movement in the 1960s. But experimentation continues today to develop architectures that shelter and engage those on an expanded mental spectrum in city life.
The question of mental health remains a key part of the discourse among architects, who have long sought to foster psychological well-being through design. At the turn of the 20th century in Vienna, architect Camillo Sitte diagnosed the modern city as producing agoraphobia, in the very moment and place where the disorder was first identified. Sitte presented his urban design, inspired by the eccentric narrow streets and small plazas of medieval cities, as a psychological counter. In the late 1940s and 1950s, Richard Neutra fashioned himself as a shrink to his clients, understood as patients.
Likewise, when the concept of stress was identified in the 1960s as the predominant response to modern life, experimental architects such as Coop Himmelb(l)au collaborated with psychiatrists to develop prototypes of relaxation architecture. Hans Hollein replaced buildings altogether with an “architecture pill” providing the desired mental state. Some mental states, such as autism, are now seen as having a spatial dimension, implying an alternative architecture in their own right.
In addition to architectures for an expanded mental spectrum, there is a need to embrace an expanded understanding of the physical spectrum. The diverse abilities of children, the elderly, amputees, the deaf, the blind, and the infirm call for greater hospitality, opportunity, and pleasure from architecture, redefining the very concept of care and transforming the role of buildings in ways that affect far more than those being treated. Aino and Alvar Aalto offered a crucial paradigm shift by arguing that architects should always design for the person in the “weakest position.”
The radicality of this proposition lies in rethinking architecture from the perspective of vulnerability itself. We must consider sickness not an exception but the norm in which different degrees of sickness define the human condition. Architecture, by this logic, is both a means of warding off the diseases of the past and producing those of the future.
Beatriz Colomina is Howard Crosby Butler Professor of the History of Architecture, the Director of Graduate Studies in the School of Architecture, and the founding director of the Interdisciplinary Media and Modernity program at Princeton University. A recipient of the Ada Louise Huxtable Prize, she is the author of many books and, most recently, the coeditor of “Radical Pedagogies” and “Sick Architecture,” from which this article is adapted.



