A Hole in the Head: A History of Trepanation
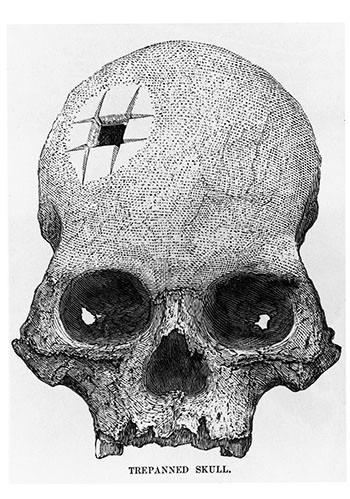
In 1865, in the ancient Inca city of Cuzco, Ephraim George Squier, explorer, archeologist, ethnologist and U.S. charge d’affaires in Central America, received an unusual gift from his hostess, Señora Zentino, a woman known as the finest collector of art and antiquities in Peru. The gift was a skull from a vast nearby Inca burial ground. What was unusual about the skull was that a hole slightly larger than a half-inch square had been cut out of it. Squier’s judgment was that the skull hole was not an injury but was the result of a deliberate surgical operation known as trepanning and furthermore, that the individual had survived the surgery.
More Tales in the History of Neuroscience.“
When the skull was presented to a meeting of the New York Academy of Medicine, the audience refused to believe that anyone could have survived a trephining operation carried out by a Peruvian Indian. Aside from the racism characteristic of the time, the skepticism was fueled by the fact that in the very best hospitals of the day, the survival rate from trephining (and many other operations) rarely reached 10 percent, and thus the operation was viewed as one of the most perilous surgical procedures. The main reason for the low survival rate was the deadly infections then rampant in hospitals. Another was that the operation was only attempted in very severe cases of head injury.
Squier then brought his Peruvian skull to Europe’s leading authority on the human skull, Paul Broca, professor of external pathology and of clinical surgery at the University of Paris and founder of the first anthropological society. Today, of course, Broca is best known for his localization of speech in the third frontal convolution, “Broca’s area,” the first example of cerebral localization of a psychological function, but at this time his fame seems to have been primarily for his craniometric and anthropological studies.
Broca and More Skulls
After examining the skull and consulting some of his surgical colleagues, Broca was certain that the hole in the skull was due to trephination and the patient had survived for a while. But when, in 1876, Broca reported these conclusions to the Anthropological Society of Paris, the audience, as in the United States, was dubious that Indians could have carried out this difficult surgery successfully.
Seven years later a discovery was made in central France that confirmed Broca’s interpretation of Squier’s skull, or at least demonstrated that “primitives,” indeed Neolithic ones, could trephine successfully. A number of skulls in a Neolithic gravesite were found with roundish holes two or three inches wide. The skulls had scalloped edges as if they had been scraped with a sharp stone. Even more remarkable, discs of skull of the same size as the holes were found in these sites. Some of the discs had small holes bored in them, perhaps for stringing as amulets. Although a few of the discs had been chiseled out after death, in most cases it was clear from the scar formation at the wound’s edge that the interval between surgery and death must have been years. Trephined skulls were found of both genders and of all ages. Virtually none of the skull holes in this sample were accidental, pathological, or traumatic. Furthermore very few of the skulls showed any sign of depressed fractures, a common indication for trephining in modern times.
Trephined skulls have been discovered in widespread locations in every part of the world, in sites dating from the late Paleolithic to this century.
These findings finally established that Neolithic man could carry out survival trephination but left unresolved the motivation for this operation. At first, Broca thought that the practice must have been some kind of religious ritual, but later he concluded that, at least in some cases, it must have had therapeutic significance. Broca actually wrote more papers on prehistoric trephination and its possible motivation than he did on the cortical localization of language. Since Broca’s time thousands of trephined skulls have been found and almost as many papers written about them. They have been discovered in widespread locations in every part of the world in sites dating from the late Paleolithic to this century. The usual estimates for survival of different samples of trephined skulls range from 50 percent to 90 percent with most estimates on the higher side.
Methods of Trephining
Across time and space five main methods of trephination were used. The first was rectangular intersecting cuts as in Squier’s skull. These were first made with obsidian, flint, or other hard stone knives and later with metal ones. Peruvian burial sites often contain a curved metal knife called a tumi, which would seem to be well suited for the job. (The tumi has been adopted by the Peruvian Academy of Surgery as its emblem.) In addition to Peru, skulls trephined with this procedure have been found in France, Israel, and Africa.
The second method was scraping with a flint as in skulls found in France and studied by Broca. Broca demonstrated that he could reproduce these openings by scraping with a piece of glass, although a very thick adult skull took him 50 minutes “counting the periods of rest due to fatigue of the hand.” This was a particularly common method and persisted into the Renaissance in Italy.
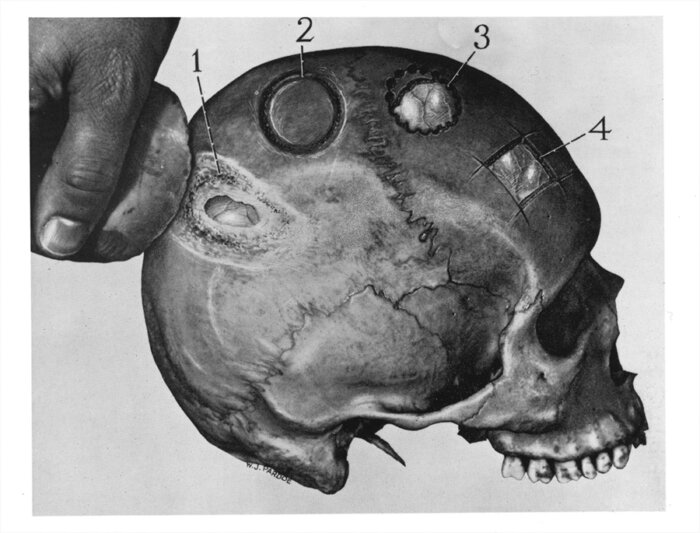
The third method was cutting a circular groove and then lifting off the disc of bone. This is another common and widespread method and was still in use, at least until recently, in Kenya.
The fourth method, the use of a circular trephine or crown saw, may have developed out of the third. The trephine is a hollow cylinder with a toothed lower edge. Its use was described in detail by Hippocrates. By the time of Celsus, a first-century Roman medical writer, it had a retractable central pin and a transverse handle. It looked almost identical to modern trephines including the one I used as a graduate student on monkeys.
The fifth method was to drill a circle of closely-spaced holes and then cut or chisel the bone between the holes. A bow may have been used for drilling or the drill simply rotated by hand. This method was recommended by Celsus, was adopted by the Arabs, and became a standard method in the Middle Ages. It is also reported to have been used in Peru and, until recently, in North Africa. It is essentially the same as the modern method for turning a large osteoplastic flap in which a Gigli saw (a sharp-edged wire) is used to saw between a set of small trephined or drilled holes. (I used this method as a graduate student, too.)
“Trepan” Versus “Trephine”
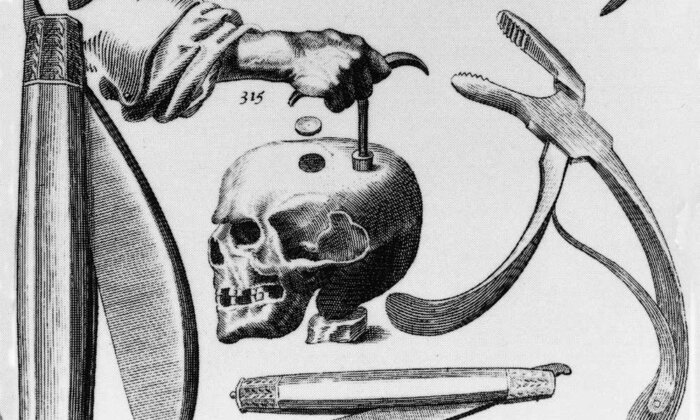
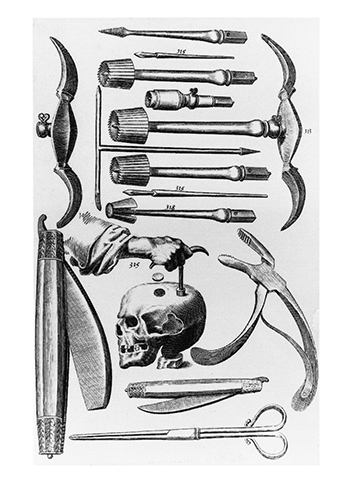
The relationship between the terms trepan and trephine is a curious one. The terms are now synonyms but have different origins and once had different meanings. In Hippocrates’ time the terms terebra and trepanon (from the Greek trupanon, a borer) were used for the instrument that is very similar to the modern trephine. In the 16th century, Fabricius ab Aquapendente invented a triangular instrument for boring holes in the skull. (He was Harvey’s teacher and the discoverer of venous valves.) It had three arms with different-shaped points. Each of the ends could be applied to the skull using the other two as handles. He called it a “tre fines” from the Latin for three ends, which became trafine and then trephine, and by 1656 it was used as a synonym for trepan, as a term for the older instrument. In another version of the etymology, a quite different triangular instrument for boring a hole in the skull was invented in 1639 by John Woodall, a London surgeon, who also called his instrument a tres fines, which became trefina and then trephine and, eventually, a synonym for trepan. More generally, in Renaissance times and later, trephination was a popular operation and a great variety of instruments for carrying it out were invented.
Why did so many cultures in different periods cut or drill holes in the skull? Since most trephined skulls come from vanished nonliterate cultures, the problem of reconstructing the motivations for trephining in these cultures is a difficult one. However, there is information about trephining in Western medicine from the fifth century BCE onward as well as about trephining in recent and contemporary non-Western medical systems. Both of these sources may throw light on the reasons for the practice in earlier times. In the following sections we consider trephination in Hippocratic medicine, in ancient Chinese medicine, in European medicine from the Renaissance onward, in contemporary non-Western medicine, and on the Internet today.
Greek Medicine
The earliest detailed account of trephining is in the Hippocratic corpus, the first large body of Western scientific or medical writing that has survived. Although there is no question that there was a famous physician called Hippocrates in the fifth century BCE, it is not clear which of the Hippocratic works were written by him. The most extensive discussion of head injuries and the use of trephining in their treatment is in the Hippocratic work On Wounds in the Head.
This treatise describes five types of head wounds. Interestingly, however, the only type for which trephination is not advocated is in cases of depressed fractures. Even when there is not much sign of bruising, drilling a hole in the head is recommended. The trephining instrument was very similar to the modern trephine, except that it was turned between the hands or by a bow and string rather than by using a crosspiece. The Hippocratic writer stressed the importance of proceeding slowly and carefully in order to avoid injuring the [dural] membrane. Additional advice was to “plunge [the trephine] into cold water to avoid heating the bone . . . often examine the circular track of the saw with the probe. . . . [and] aim at to and fro movements.” Trephining over a suture was to be studiously avoided.
The Hippocratic doctors believed that stagnant blood (like stagnant water) was bad. It could decay and turn into pus. Thus, the reason for trephining, or at least one reason, was to allow the blood to flow out before it spoiled.
Apparently the Hippocratic doctors expected bleeding from a head wound and the reason for drilling the hole in the skull was to allow the blood to escape (“let blood by perforating with a small trepan, keeping a look out [for the dura] at short intervals”). Since they presumably had no notion of intracerebral pressure, why did they want the blood to run out? Although the reasons for trephining are not discussed in “On Wounds in the Head,” they seem clear from other Hippocratic treatises such as “On Wounds and On Diseases.” The Hippocratic doctors believed that stagnant blood (like stagnant water) was bad. It could decay and turn into pus. Thus, the reason for trephining, or at least one reason, was to allow the blood to flow out before it spoiled. In cases of depressed fractures, there was no need to trephine since there were already passages in the fractured skull for the blood to escape.
By Galen’s time (129–199) trephining was in standard use in treating skull fracture for relieving pressure, for gaining access to remove skull fragments that threatened the dura, and, as in Hippocratic medicine, for drainage. Galen discussed the techniques and instruments in detail and advocated practicing on animals, especially the Barbary “ape” (Macaca sylvana). He was well aware of avoiding damage or pressure on the dura and indeed carried out experiments on the effect of pressing on the dura in animals.
Trepanation in Ancient China
The possibility that trepanation was practiced in ancient China is suggested by the following story about Cao Cao and Hua Tua, from a historical novel attributed to Luo Guanzhong, written in the Ming dynasty (1368–1644) and set in 168–280 at the end of the Later Han dynasty. Cao Cao was commander of the Han forces and posthumously Emperor of the Wei dynasty, and Hua Tuo was (and still is) a famous physician of the time.
Cao Cao screamed and awoke, his head throbbing unbearably. Physicians were sought, but none could bring relief. The court officials were depressed. Hua Xin submitted a proposal: “Your highness knows of the marvelous physician Hua Tuo? . . . Your highness should call for him.”
Hua Tuo was speedily summoned and ordered to examine the ailing king. “Your Highness’s severe headaches are due to a humor that is active. The root cause is in the skull, where trapped air and fluids are building up. Medicine won’t do any good. The method I would advise is this: after general anesthesia I will open your skull with a cleaver and remove the excess matter, only then can the root cause be removed.” “Are you trying to kill me?” Cao Cao protested angrily . . . [and] . . . ordered Hua Tuo imprisoned and interrogated.
Ten days later Hua Tuo died. His medical text was lost upon his death.
Western Medicine
From the Renaissance until the beginning of the 19th century trephining was widely advocated and practiced for the treatment of head wounds. The most common use was in the treatment of depressed fractures and penetrating head wounds. However, because of the high incidence of mortality particularly when the dura was penetrated, there was considerable debate in the medical literature throughout this long span about if and when to trephine. Besides trephining in cases of skull fracture, the Hippocratic practice of “prophylactic trephination” in the absence of fracture after head injury continued to persist. For example, in the 1800s Cornish miners “insisted on having their skulls bored” after head injuries, even when there was no sign of fracture.
The practice of trephination was so dangerous that the first requirement for the operation was said to be “that the wound surgeon himself must have fallen on his head.”
Until the early 19th century trephination was done in the home. However, when the operation was moved to hospitals, the mortality was so high that trephination for any reason including treatment of fractures and other head injury declined precipitously. The practice was so dangerous that the first requirement for the operation was said to be “that the wound surgeon himself must have fallen on his head.” Or as Sir Astley Cooper put it in 1839, “If you were to trephine you ought to be trephined in turn.” It was against this background that the discovery of Neolithic trephining was so unbelievable to the American and French medical communities in the middle of the 19th century. Eventually, the introduction of modern antisepsis and prophylaxis of infection at the end of the 19th century, as well as an increased understanding of the importance of intracerebral pressure in head injury, allowed trephination to return as a common procedure in the management of head trauma.
In modern neurosurgical practice, trephining is still an important procedure but it is no longer viewed as therapeutic in itself. It may be used for exploratory diagnosis, for relieving intracerebral pressure (as from an epidural or subdural hematoma), for debridement of a penetrating wound, and to gain access to the dura and thence the brain itself (for example, to provide a port through which a stereotactic probe can be introduced into the brain.)
Epilepsy and Mental Disease
In the European medical tradition, in addition to its use in treating head injury, trephining has been an important therapy for two other conditions, epilepsy and mental illness.

The tradition of trephining as a treatment for epilepsy begins as early as Aretaeus the Cappadocian (ca. 150), one of the most famous Greek clinicians, and lasted into the 18th century. The 13th-century surgical text “Quattuor magistri” recommended opening the skulls of epileptics so “that the humors and air may go out and evaporate.” However, by the 17th century trephination for epilepsy was beginning to be viewed as an extreme measure, as in Riverius, “The Practice of Physick” (1655):
If all means fail the last remedy is to open the fore part of the Skul with a Trepan, at distance from the sutures, that the evil air may breath out. By this means many desperate Epilepsies have been cured, and it may be safely done if the Chyrurgeon be skilful.
One 13th-century text recommended opening the skulls of epileptics so “that the humors and air may go out and evaporate.”
By the 18th century the incidence of trephining for epilepsy had declined and its rationale changed. Now rather than the idea of allowing an exit for evil vapors and humors, the purpose was to remove some localized pathology. By the 19th century trephining for epilepsy was confined to the treatment of traumatic epilepsy, that is, cases associated with known head injury.
Another use of trephining was as a treatment for mental disease. In his “Practica Chirurgiae,” Roger of Parma (ca. 1170) wrote:
For mania or melancholy a cruciate incision is made in the top of the head and the cranium is penetrated, to permit the noxious material to exhale to the outside. The patient is held in chains and the wound is treated, as above, under treatment of wounds.
Robert Burton, in “Anatomy of Melancholy” (1652), also advocated boring a cranial hole for madness, as did the great Oxford neuroanatomist and physician Thomas Willis (1621–1675).

Probably the most famous depictions of apparent trephining for mental disease are in early Flemish Renaissance painting. Thus, Hieronymus Bosch’s The Cure for Madness (or Folly), also known as The Stone Operation, shows a surgical incision being made in the scalp. The inscription has been translated in part “Master, dig out the stones of folly.” There are similar depictions of the removal of stones from the head by Peter Bruegel, Jan Steen, Pieter Huys, and other artists of the time.
By the 18th century, “most reputable and enlightened surgeons gave up the practice of . . . [trephination] . . . for psychiatric aberrations or headache without evidence of trauma. Thus, . . . the skull was never to be trephined for ‘internal disorders of the head.”’
Trephining in Africa
Herodotus describes the Libyans as cauterizing the heads of their children to “prevent them being plagued in their afterlives by a flow of rheum from the head.” And indeed, trephined skulls have been found among the people he was probably writing about, the Tuareg nomads.
An important source of information on the motivations for trephination is contemporary traditional practitioners and their patients. There are literally hundreds of 20th-century accounts of trephination, particularly in Oceanic and African cultures. Especially detailed and recent ones concern the Kisii of South Nyanza in Kenya and include photographs of the surgical instruments, practitioners, and patients; X-rays of the skulls of surviving patients; detailed interviews; and even a documentary film.
The ancient Greek historian Herodotus describes the Libyans as cauterizing the heads of their children to “prevent them being plagued in their afterlives by a flow of rheum from the head.”
Trephining among the Kisii is carried out primarily for the relief of headache after some kind of head injury. According to Margetts, it is not done for “psychosis, epilepsy, dizziness or spirit possession.” The operation is carried out by general practitioners of medicine and takes a few hours. Restraint rather than anesthesia is used. The hole in the skull is usually made by scraping with a sharp knife with a curved tip to avoid injuring the dura. Various medicines are administered before, during, and after surgery but their nature does not seem to have been studied. Mortality, by one authority, is described as “low, perhaps 5 per cent.” The practitioners and patients seem to be quite satisfied with the results of the operation.
Although headache after head injury is the most prevalent reason given for trephining by contemporary practitioners of traditional medicine in Africa and elsewhere, other reasons are cited in the literature such as “to let out the evil spirits which were causing an intractable headache.”
Trephining on the Internet
Today, the practice of trephining is not confined to surgical suites or traditional medicine men. It is advocated by the International Trepanation Advocacy Group as a means of enlightenment and enhanced consciousness. Their general idea is that when the skull sutures close in childhood it “inhibits brain pulsations causing a loss of dreams, imagination and intense perceptions.” Trephining a small hole, they say, “restores the intracranial pulse pressure which leads to a permanent increase of the brain-blood volume which leads to accelerated brain metabolism and more areas of the brain functioning simultaneously” and “increased originality, creativity and…testosterone level.” Beyond such “physiological” arguments, the group supports the practice by pointing out its ancient, widespread, and continuing presence in other cultures. This particular form of alternative medicine recently gained considerable if not entirely positive publicity: In November 1998 it was featured on ER, the television soap opera set in an emergency ward.
Much of the defense for alternative medicine treatments is that they must work because they have been around for such a long time, an apparently attractive argument for the increasing popularity of five-thousand-plus-year-old Chinese traditional medical practices. However, the case of trephining suggests that just because a procedure is very old does not mean it is necessarily an effective one, at least for enhanced enlightenment and creativity.
Trepanation as an Empirical If Not a Rational Procedure
The most common view of the prehistoric and the non-Western practice of trephining, especially in the absence of a depressed fracture, was that it represented some kind of “superstition,” “primitive thinking,” “magic,” or “exorcism.” Yet an examination of the reasons for the practice among the Hippocratic and early European doctors as well as among contemporary Kenyan practitioners suggests a different view. Trephining may have appeared, in these contexts and cultures, to have been an effective empirical approach to head injury and the headaches that often accompany them. Headaches after head injury often do feel like “a pounding” and “pressure” inside the head and thus the idea that a hole in the skull would relieve them is not necessarily magical or bizarre. Furthermore, epidural bleeding does sometimes accompany head injury, and in these cases trephining might have actually reduced intracranial pressure. Finally, the apparently excellent survival rate meant that the procedure, at least until it moved into a hospital setting, may have met the prime requirement of medicine, “do no harm.”
POSTSCRIPT
The first International Colloquium on Cranial Trepanation in Human History was held at the University of Birmingham in April 2000. Papers from this unique three-day meeting were published as Trepanation: History, Discovery, Theory, which provides the most complete review of the subject to date. A major achievement of the meeting was the demonstration that trepanation was widespread in many regions of Europe, Asia, Africa, Oceania, and the Americas in both preliterate and literate periods. The volume also contains illustrations of trephined skulls from many cultures and of the great variety of instruments used.
Another interesting development was the return of E. L. Margetts to the Kisii of Kenya, whose trepanning practices he had studied 25 years earlier. He estimates that there may now be more than 100 surgeons carrying out the operation. Unlike in the past, they now use modern Western local anesthetics injected into the scalp prior to surgery. However, the reasons for the very low rate of infections still have not been studied systematically.
Since my original article, there seems to have been an increase in Internet sites advocating trepanning and often self-trepanning for the treatment of, among other disorders, depression, chronic fatigue syndrome, and stress and to improve mental “energy and vigor.”
The British Medical Journal took these developments seriously enough to issue a warning of their dangers:
Doctors have warned about the dangers of trepanning after the launch of several websites promoting the “do it yourself ” surgery and the case of a Gloucestershire woman who drilled a 2 cm diameter hole in her skull. Concern has been expressed about the growing interest in trepanning for several conditions, including depression and chronic fatigue syndrome. Concern is also growing about the increasing promotion of trepanning, including videos, T-shirts, and a virtual trepanning shopping mall on the internet.
Trepanning received widespread publicity when the surgeon Stephen Maturin carried out the procedure on a sailor in view of the assembled crew in the film Master and Commander: The Far Side of the World, based on the Patrick O’Brian naval novels about the Napoleonic Wars.
Charles G. Gross was a pioneering neuroscientist who specialized in vision and the functions of the cerebral cortex. This essay is excerpted from his book “A Hole in the Head: More Tales in the History of Neuroscience.”